Local Anesthesia in Pediatric Dental GA Cases
Survey Results
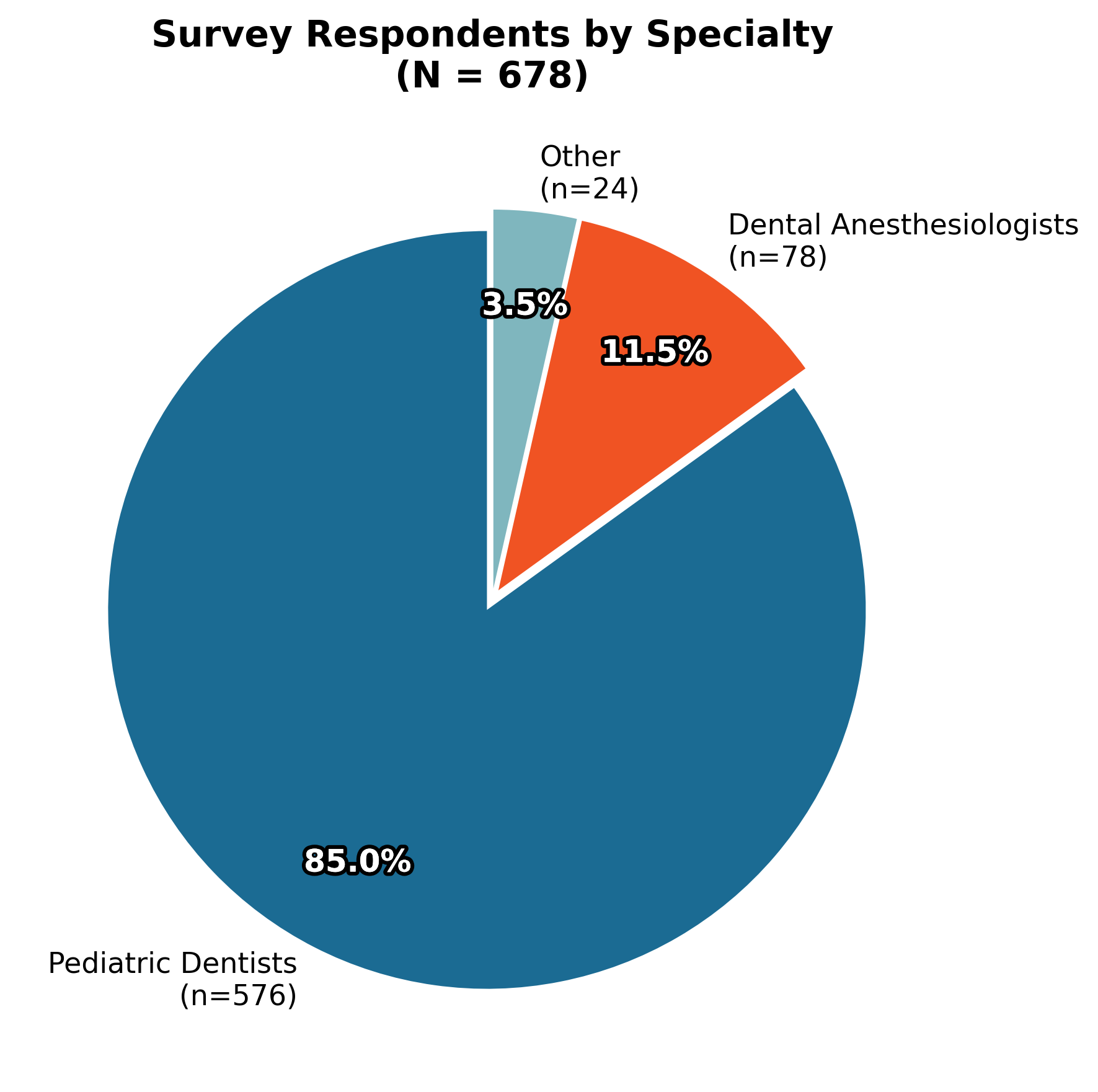
678
Total Respondents
576
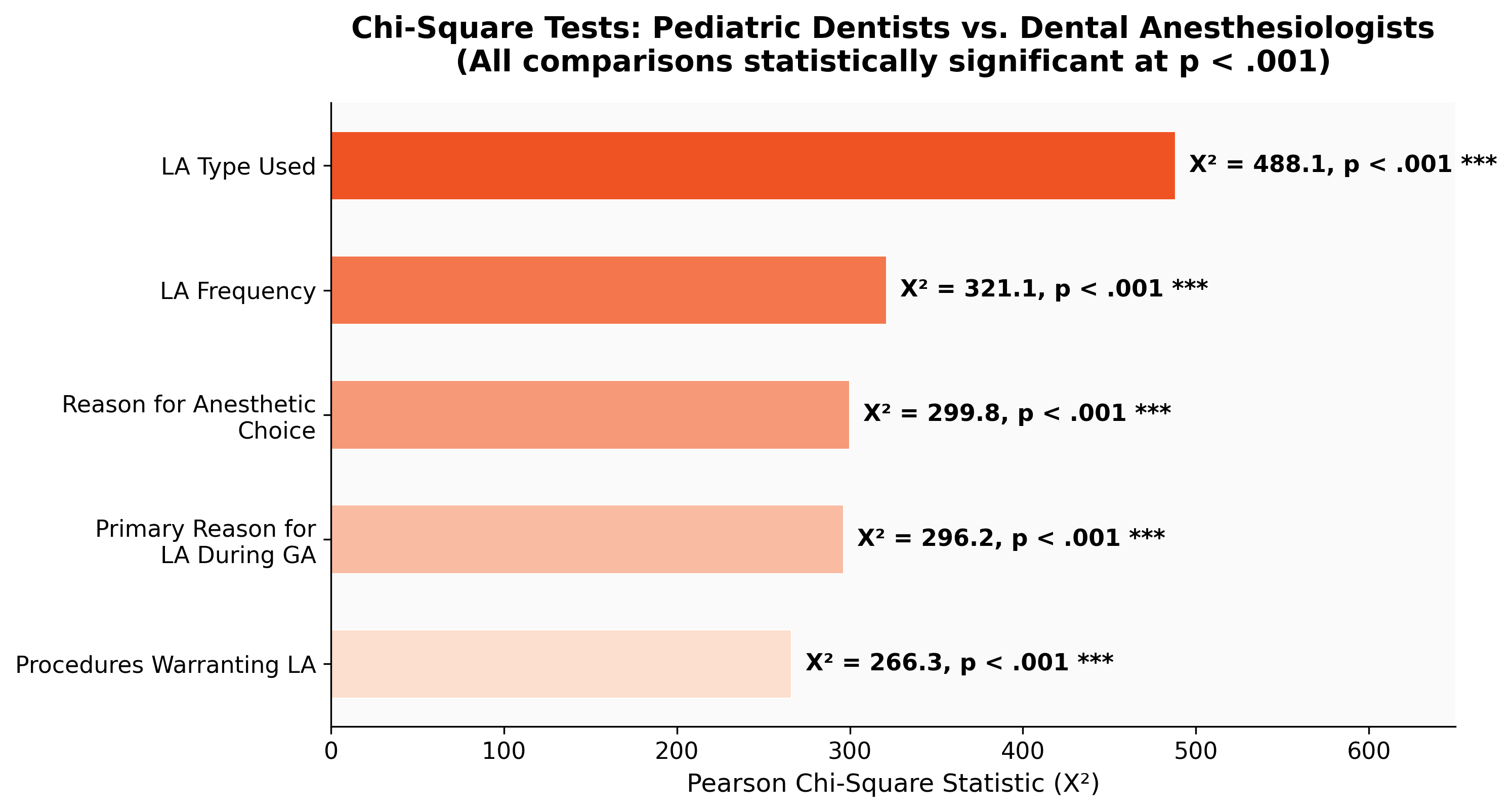
Pediatric Dentists
78
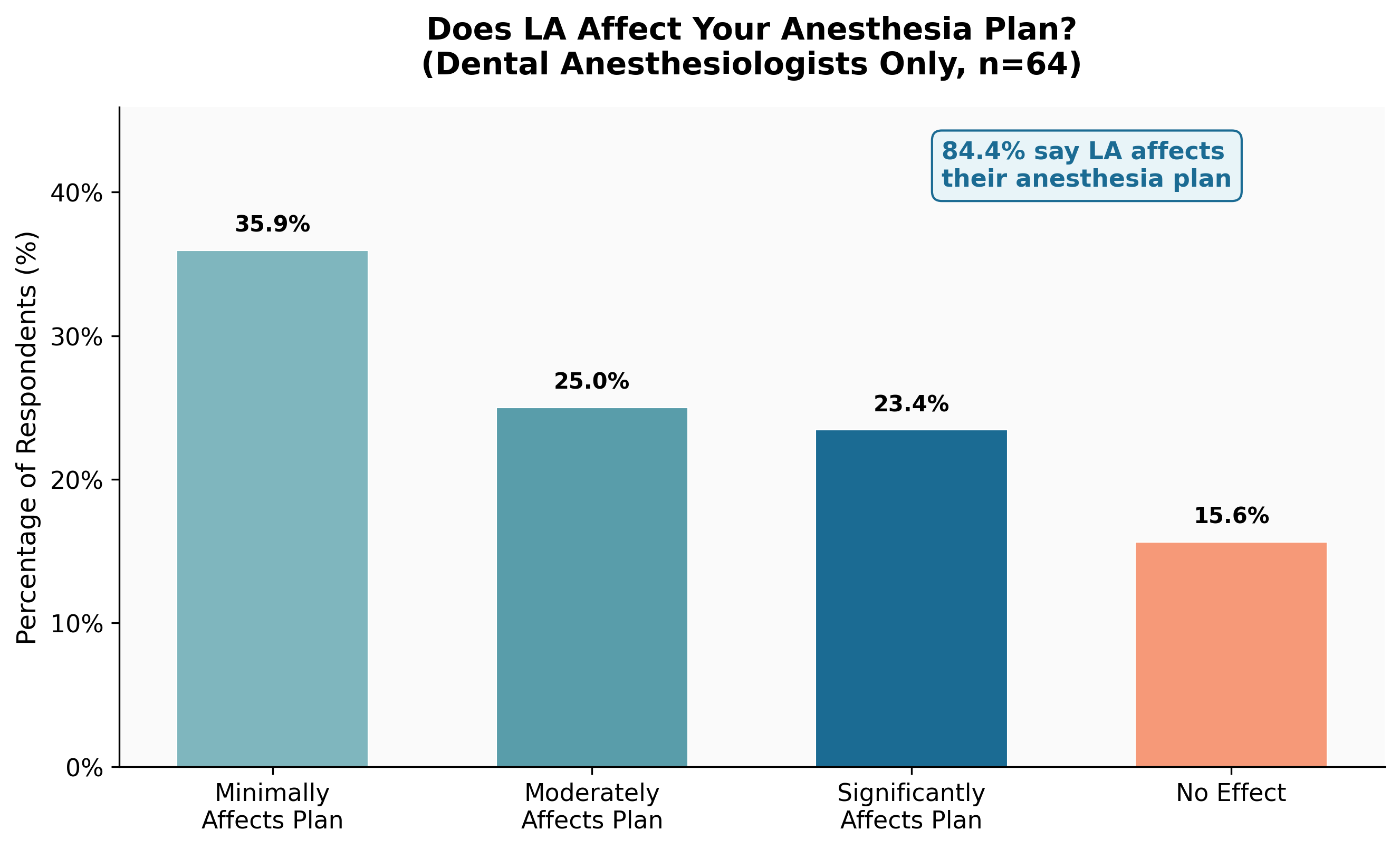
Dental Anesthesiologists
14
Charts
Demographics
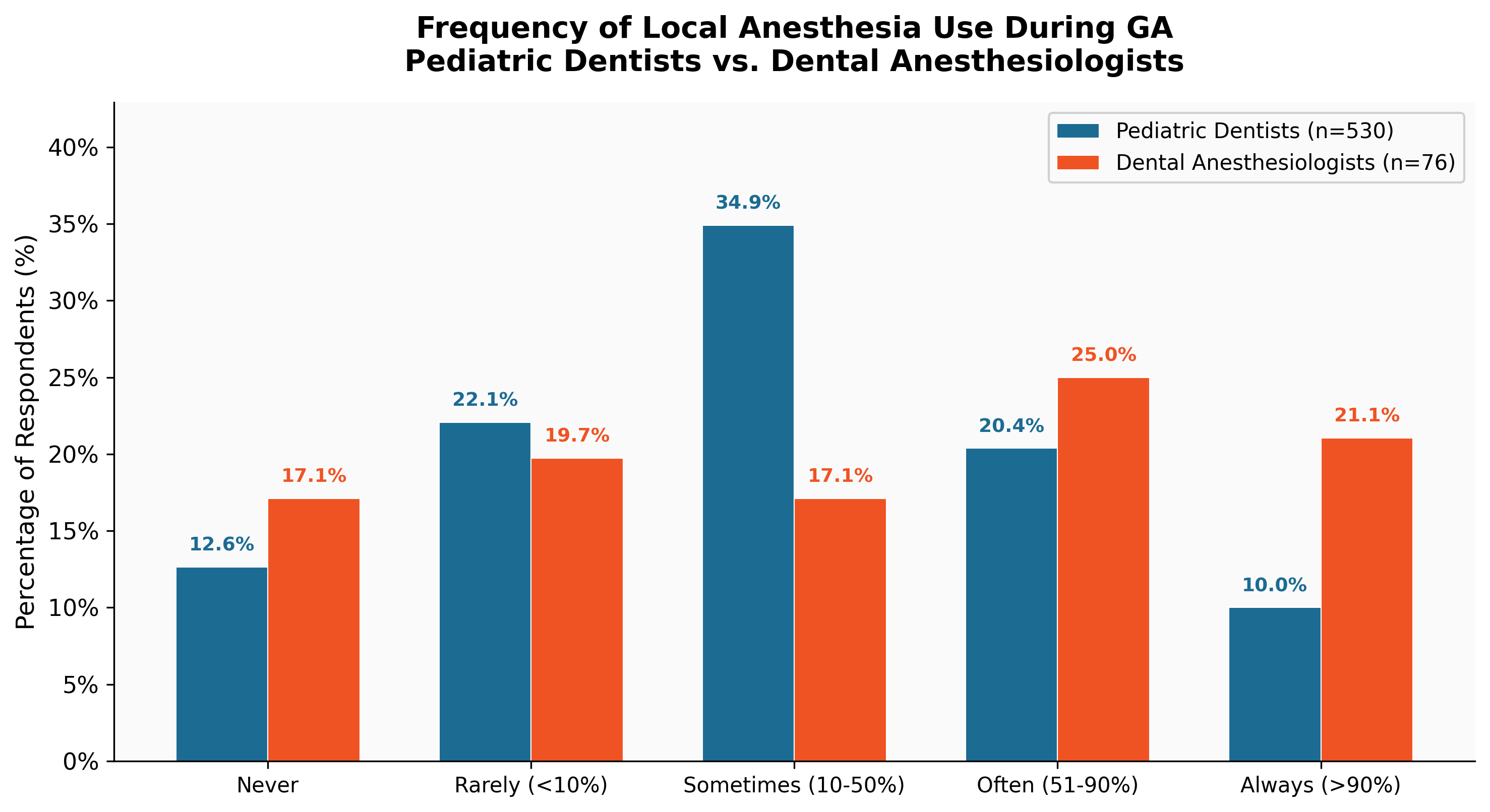
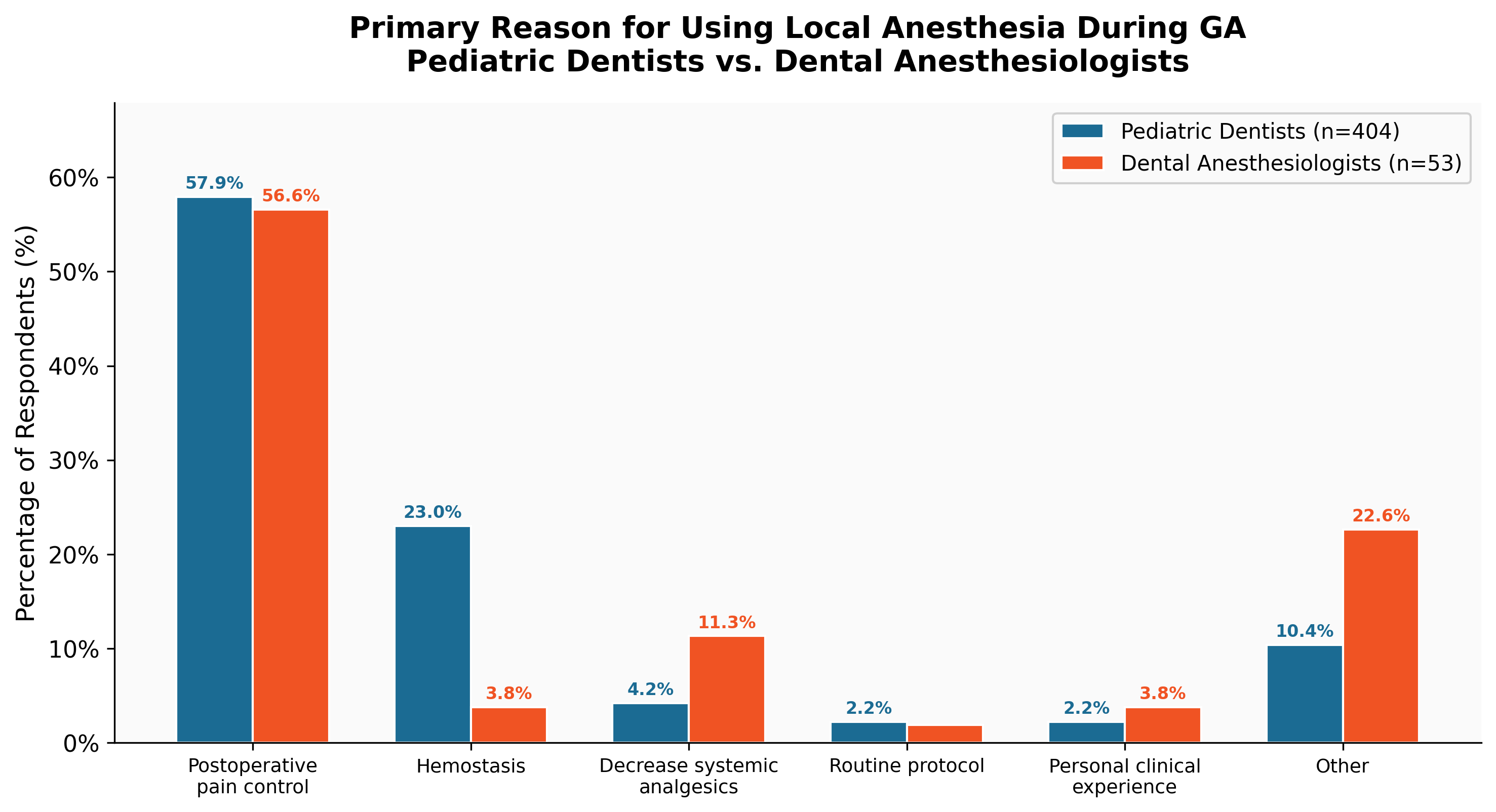
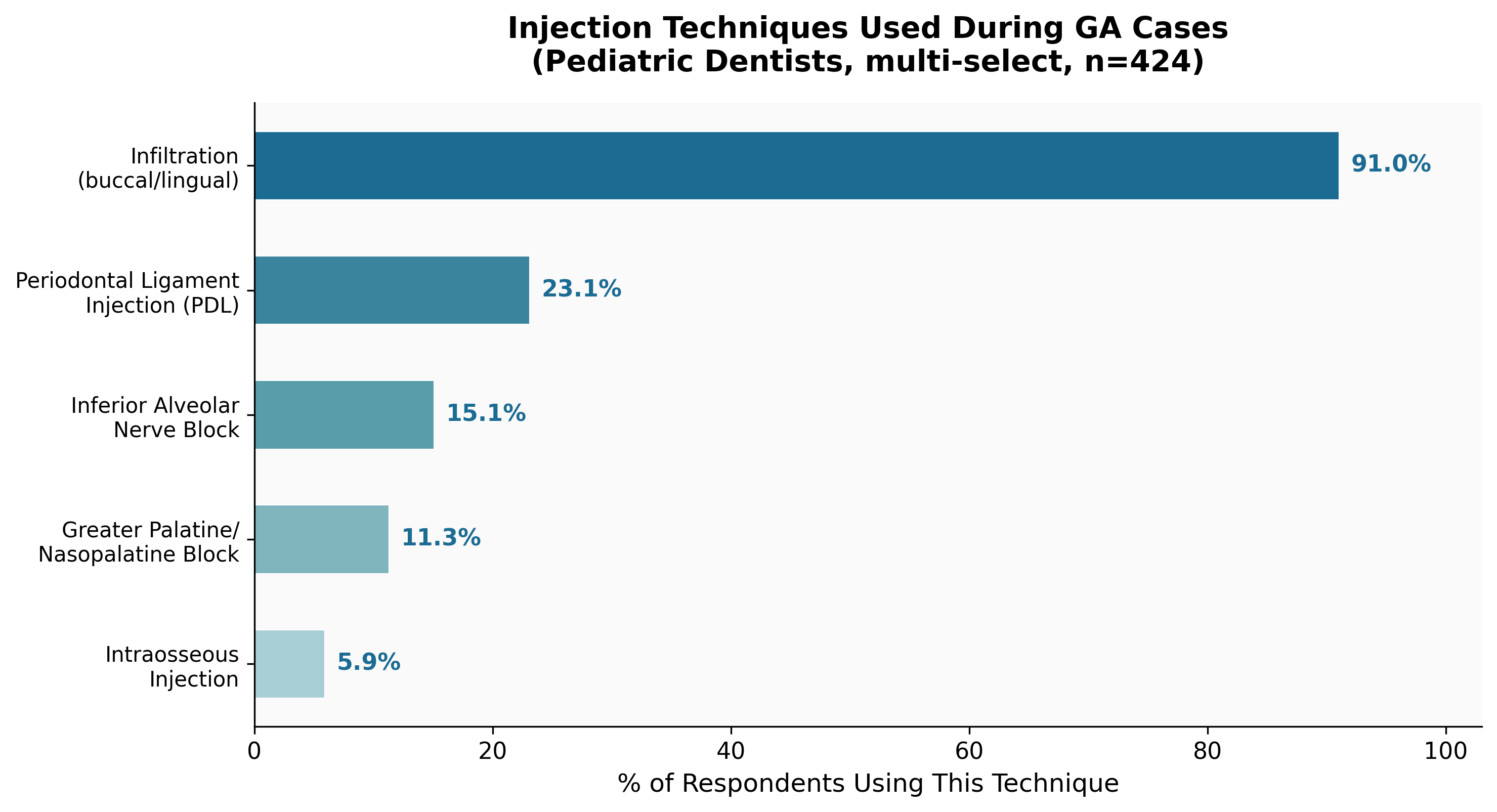
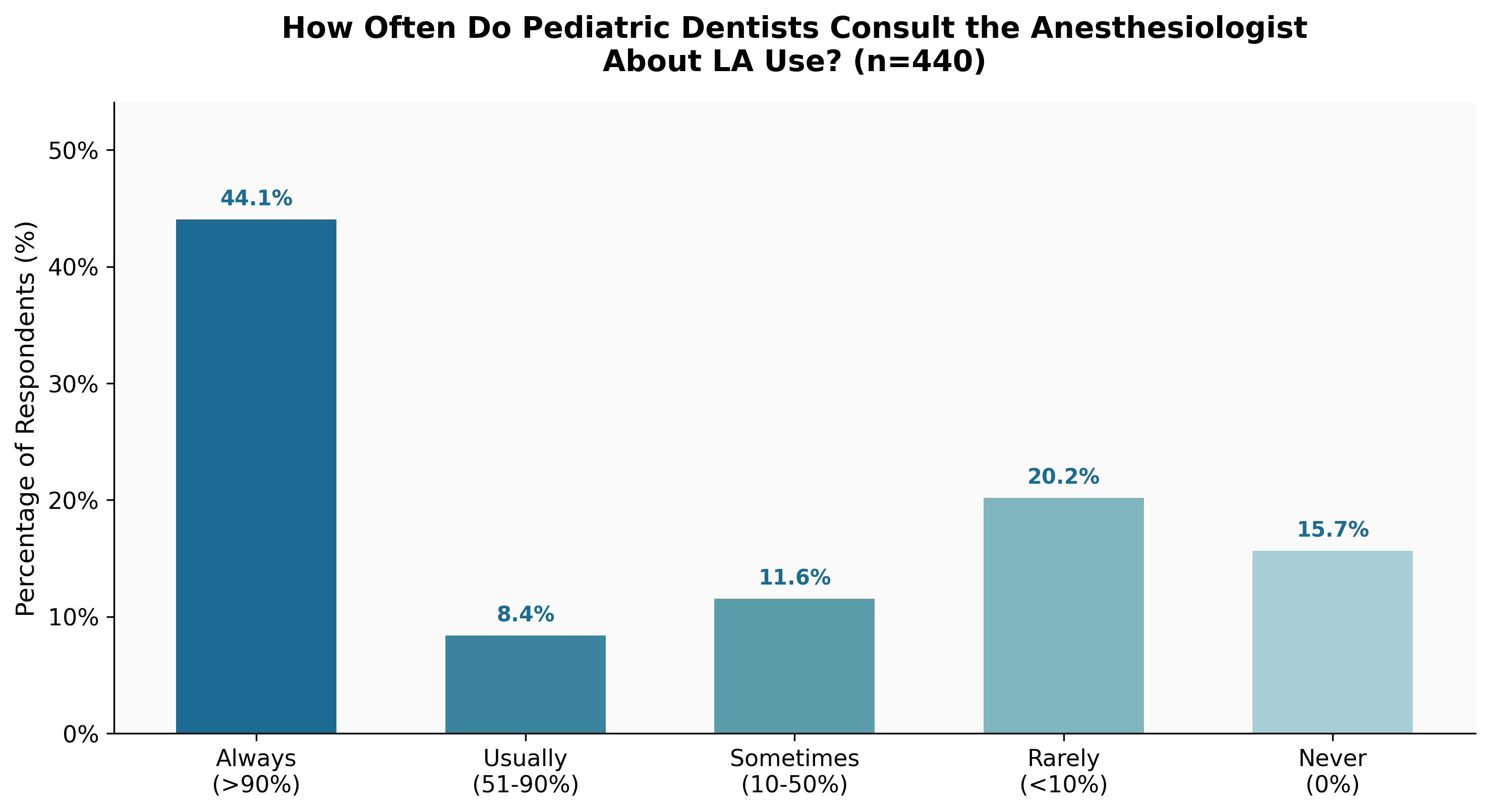
Local Anesthesia Use Patterns
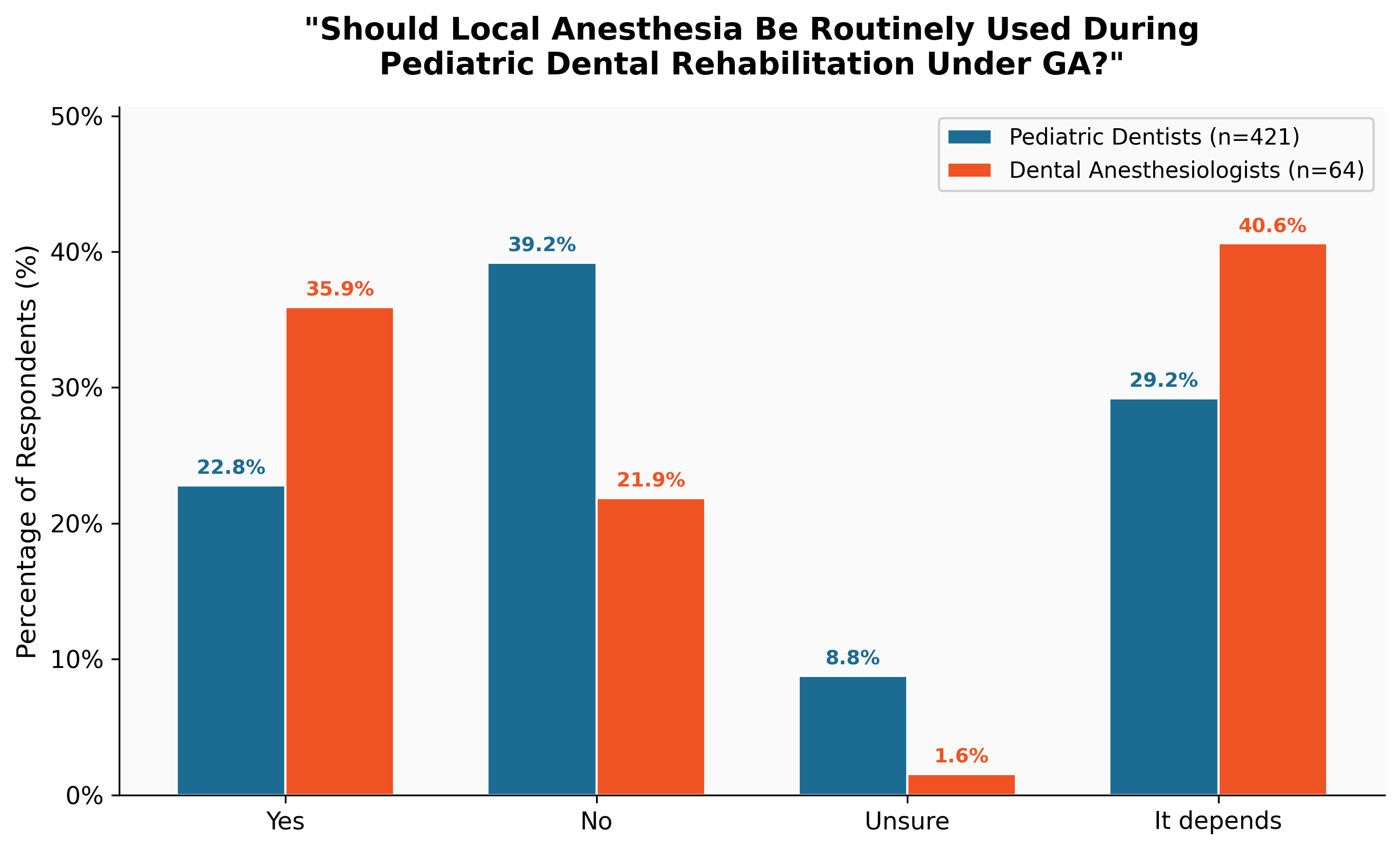
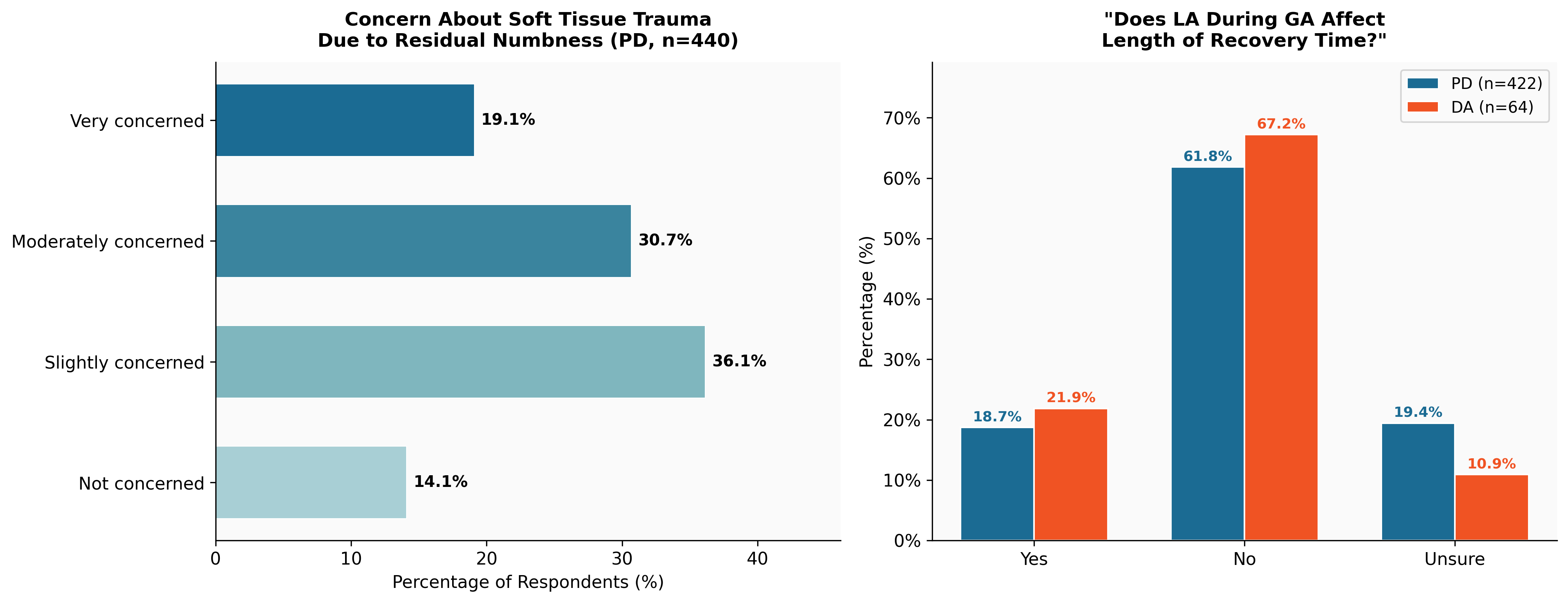
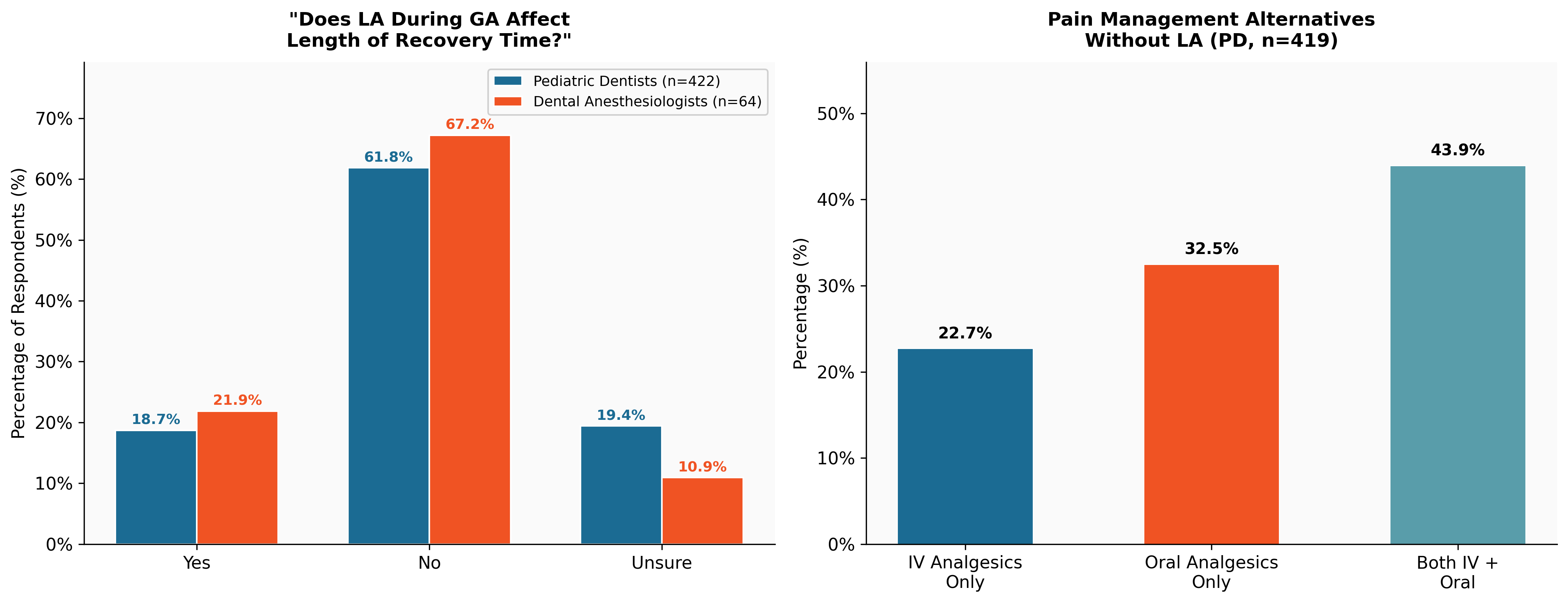
Clinical Opinions and Outcomes
Concerns and Decision Factors
Statistical Analysis